
Effect of co-trimoxazole prophylaxis on morbidity and mortality of HIV-exposed, HIV-uninfected infants in South Africa: a randomised controlled, no…
Authors of this article are:
Daniels B, Coutsoudis A, Moodley-Govender E, Mulol H, Spooner E, Kiepiela P, Reddy S, Zako L, Ho NT, Kuhn L, Ramjee G.
A summary of the article is shown below:
BACKGROUND: WHO guidelines recommend co-trimoxazole prophylaxis for HIV-exposed, HIV-uninfected infants. These guidelines date back to an era in which HIV testing of infants was impossible and mothers had poor access to antiretroviral treatment. To determine whether this guideline requires revision in the current era of effective prevention of mother-to-child transmission and early infant diagnosis programmes, we aimed to investigate whether receiving no co-trimoxazole prophylaxis is inferior to receiving co-trimoxazole prophylaxis in the resulting incidence of grade 3 or 4 common childhood illnesses or mortality in breastfed HIV-exposed, HIV-uninfected infants.METHODS: We investigated our aim in a randomised controlled, non-inferiority trial. We enrolled the HIV-negative infants of mothers living with HIV who were actively involved in transmission prevention programmes in two clinics in Durban, South Africa. Infants were included in the study if they were breastfeeding at the screening and enrolment visits, and their mother was planning to breastfeed for at least 6 months; were a singleton birth and had a birthweight of 2 kg or more; had no clinically observed genetic disorders; and had no serious illnesses and had not received antibiotics or traditional medications (such as herbal remedies). Infants were randomly assigned (1:1) to receive co-trimoxazole or no co-trimoxazole. In the co-trimoxazole group, infants received the drug until all exposure to HIV had ceased (ie, 6 weeks after last exposure to breastmilk) and the infant was confirmed to be uninfected with HIV. The drug was administered by mothers in once-daily regimens of 20 mg trimethoprim and 100 mg sulfamethoxazole orally (age <6 months or bodyweight <5 kg), or 40 mg trimethoprim and 200 mg sulfamethoxazole orally (age >6 months or bodyweight >5 kg). Clinical and laboratory staff always remained masked to group assignment, but mothers and study counsellors were not. Infants and their mothers attended study visits at ages 6 weeks (for enrolment and randomisation), 10 weeks, 14 weeks, and then monthly from 4 to 12 months. Our primary outcome was the incidence of grade 3 or 4 common childhood illnesses (pneumonia or diarrhoea) or mortality in breastfed HIV-exposed, HIV-uninfected infants by age 12 months. A non-inferiority bound of 5% was used. The study is registered with the Pan African Clinical Trials Registry, number PACTR201311000621110, and the South African National Clinical Trials Registry, number DOH-27-0614-4728.FINDINGS: We screened 1570 mother-child pairs for study enrolment, from whom (78%) eligible infants were enrolled into the study between Oct 16, 2013, and May 23, 2018. Of the infants enrolled, 611 (50%) were randomly assigned to the co-trimoxazole group and 609 (50%) were randomly assigned to the no co-trimoxazole group. One (<1%) infant in the no co-trimoxazole group was excluded from the analysis of the final outcomes for having received traditional medicine (which only became apparent after randomisation); therefore, 611 (50%) infants in the co-trimoxazole group and 608 (50%) infants in the no co-trimoxazole group were included in the final intention-to-treat analysis. 136 (22%) infants in the co-trimoxazole group and 139 (23%) infants in the no co-trimoxazole group did not complete the 12-month study visit, predominantly because of loss to follow-up (93 [15%] infants in the co-trimoxazole group; 90 [15%] infants in the no co-trimoxazole group). The cumulative probability of the composite primary outcome was 0·114 (95% CI 0·076 to 0·147; 49 events) in the co-trimoxazole group versus 0·0795 (0·044 to 0·115; 39 events) in the no co-trimoxazole group. The risk difference (no co-trimoxazole group minus co-trimoxazole group) was -0·0319 (-0·075 to 0·011), meaning that the risk was around 3 percentage points lower in the no co-trimoxazole group on the additive scale.INTERPRETATION: We can conclude that no co-trimoxazole is not inferior to daily co-trimoxazole among breastfed HIV-exposed, HIV-uninfected infants whose mothers are accessing a prevention of mother-to-child transmission programme in an area unaffected by malaria. We therefore believe that WHO should revise the co-trimoxazole guidelines for HIV-exposed, HIV-uninfected infants in areas unaffected by malaria.FUNDING: HIV Prevention Research Unit of the South African Medical Research Council and the Family Larsson-Rosenquist Foundation.Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Check out the article’s website on Pubmed for more information:
[link-preview url=https://www.ncbi.nlm.nih.gov/pubmed/31708152 forceshot=true]
This article is a good source of information and a good way to become familiar with topics such as: .
NativeFolder: The Only Bacterial Culture Medium for the Expression of Soluble Proteins
-
- Sale!
- Molecular Biology, Research Kits
NativeFolder Bacterial Culture Medium
- Original price was: $795.00.$295.00Current price is: $295.00.


Interference Test Kit for Assay Validation
-
- Sale!
- Interference, Research Kits
Interference Test Kit
- Original price was: $995.00.$495.00Current price is: $495.00.


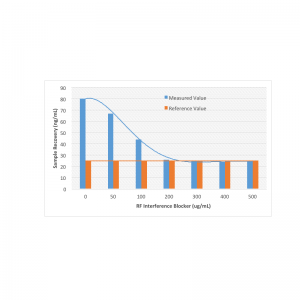
Rheumatoid Factor Interference Blocker
-
- Sale!
- Antibodies, Interference
Rheumatoid Factor Interference Blocker
- Original price was: $595.00.$395.00Current price is: $395.00.

New Antibodies from MOLECULAR DEPOT
-
- Sale!
- Antibodies
AKT1S1 Antibody
- Original price was: $1,295.00.$695.00Current price is: $695.00.
-
- Sale!
- Antibodies
PYGL Antibody (C-Term)
- Original price was: $1,295.00.$695.00Current price is: $695.00.
-
- Sale!
- Antibodies
BCL6 Antibody (C-Term)
- Original price was: $1,295.00.$695.00Current price is: $695.00.
-
- Sale!
- Antibodies
DANRE tfap2e Antibody (C-Term)
- Original price was: $1,295.00.$695.00Current price is: $695.00.
-
- Sale!
- Antibodies
TIMP2 Antibody
- Original price was: $1,295.00.$695.00Current price is: $695.00.
-
- Sale!
- Antibodies
EphB3 Antibody
- Original price was: $1,295.00.$695.00Current price is: $695.00.
-
- Sale!
- Antibodies
DCAMKL1 Antibody (C-Term)
- Original price was: $1,295.00.$695.00Current price is: $695.00.
-
- Sale!
- Antibodies
ENOG Antibody
- Original price was: $1,295.00.$695.00Current price is: $695.00.
-
- Sale!
- Antibodies
M Tfap2c Antibody (N-Term)
- Original price was: $1,295.00.$695.00Current price is: $695.00.
-
- Sale!
- Antibodies
SUMO1 Antibody (C-Term)
- Original price was: $1,295.00.$695.00Current price is: $695.00.




New Proteins from MOLECULAR DEPOT
-
- Sale!
- Conjugates, Proteins
Captopril HSA Biotin Conjugate
- Original price was: $1,995.00.$995.00Current price is: $995.00.
-
- Sale!
- Proteins
PKC-α, Active, GST-tagged from Xanopus sp.
- Original price was: $1,595.00.$795.00Current price is: $795.00.
-
- Sale!
- Conjugates, Proteins
Prilocain BSA Biotin Conjugate
- Original price was: $1,995.00.$995.00Current price is: $995.00.
-
- Sale!
- Conjugates, Proteins
T3 (Triiodothyronine) BSA Biotin Conjugate
- Original price was: $1,995.00.$995.00Current price is: $995.00.
-
- Sale!
- Conjugates, Proteins
Pipemidic Acid BSA Biotin Conjugate
- Original price was: $1,995.00.$995.00Current price is: $995.00.
-
- Sale!
- Proteins
PKD2 Protein, Active (Recombinant Human)
- Original price was: $1,795.00.$895.00Current price is: $895.00.
-
- Sale!
- Conjugates, Proteins
Meropenem BSA Biotin Conjugate
- Original price was: $1,995.00.$995.00Current price is: $995.00.
-
- Sale!
- Conjugates, Proteins
Piperacillin BSA Biotin Conjugate
- Original price was: $1,995.00.$995.00Current price is: $995.00.
-
- Sale!
- Proteins
Protein A Peroxidase from Staphylococcus aureus/horseradish
- Original price was: $1,195.00.$595.00Current price is: $595.00.
-
- Sale!
- Conjugates, Proteins
Tobramycin BSA Biotin Conjugate
- Original price was: $1,995.00.$995.00Current price is: $995.00.










New Chemicals from MOLECULAR DEPOT
-
- Sale!
- Chemicals, Interference, Lipids
Triglyceride Mix for Interference Testing
- Original price was: $895.00.$395.00Current price is: $395.00.
-
- Sale!
- Chemicals
Microparticle Stabilizer Solution
- Price range: $295.00 through $495.00
-
- Sale!
- Buffers & Solutions, Chemicals
Enzyme Acceptor Stabilization Buffer
- Original price was: $495.00.$250.00Current price is: $250.00.
-
- Sale!
- Buffers & Solutions, Chemicals
Enzyme Donor Stabilization Buffer
- Original price was: $495.00.$250.00Current price is: $250.00.
-
- Sale!
- Chemicals, Conjugates
Progesterone Biotin Conjugate Solution
- Original price was: $995.00.$595.00Current price is: $595.00.
-
- Sale!
- Buffers & Solutions, Chemicals
Microparticle Activation Buffer
- Price range: $395.00 through $695.00
-
- Sale!
- Buffers & Solutions, Chemicals
Microparticle Washing Buffer
- Price range: $395.00 through $695.00
-
- Sale!
- Buffers & Solutions, Chemicals
Microparticle Blocking Buffer
- Price range: $395.00 through $695.00
-
- Sale!
- Buffers & Solutions, Chemicals
Latex Microparticles Anti Aggregation Agent
- Price range: $295.00 through $3,500.00
-
- Sale!
- Chemicals
CPRG (Chlorophenol red-β-D-galactopyranoside)
- Original price was: $850.00.$395.00Current price is: $395.00.









